
This is my first blog and would appreciate your feedback as to what you would find helpful in future blogs.
I’ve just returned from 3 weeks in beautiful Scotland. I presented our results of liposuction for advanced lymphoedema at the International Lymphology Framework meeting in Glasgow http://www.ilfconference.org/. I then went touring with my wife with lots of walking up “Bens” and along “Glens” balanced by lots of eating (and a little drinking) afterwards. I’m afraid I avoided the Haggis and Black Pudding but my wife Dianne was a lot braver. I then visited my colleague Prof Alex Munnoch at Ninewells Hospital Dundee and presented a lecture on the Impact of local control on survival after breast cancer and also attended several meetings.

I came back last Thursday to a very busy clinic and a few “urgent” fit in patients.
This week, a young woman and her husband came to see me for a second opinion. “Clare” (not her real name) felt a little let down by the medical system. She had found a copy of my book, Breast Cancer: Taking Control at her local book store and told me it had really helped her and wanted me to help her. I started writing the book in 2006 and published it on September 14, 2010 with an Ebook update in November 2013. The book was “in my head” for many years but I finally got sick and tired of some patients being mismanaged with one memorable case finally compelling me to start writing. I’ll tell you a bit more about this in a future blog.
Clare had a lump for 3 months before her diagnosis and an initial fine needle biopsy was “negative”. The lump then grew but because the initial biopsy was negative, she did not undergo a repeat ultrasound or biopsy and just proceeded with removal of the lump, a procedure called an excision biopsy.
It’s always better to have a pre-operative diagnosis as this allows us to plan surgery with greater attention to the margins of excision and also to figure out what to do about the axilla. If a repeat biopsy was done, and mucinous carcinoma diagnosed, then a wide local excision and sentinel node biopsy would have been performed. The lack of a pre-operative diagnosis meant that Clare needed another anaesthetic to widely excise the area where the mucinous cancer started and to perform a sentinel node biopsy.
The diagnosis was that of a mucinous carcinoma which usually occurs later in life. In my book, Breast Cancer: Taking Control I talk about the different types of breast cancer in the introduction. Here is an excerpt from the introduction section of my book:
Understanding your type of breast cancer
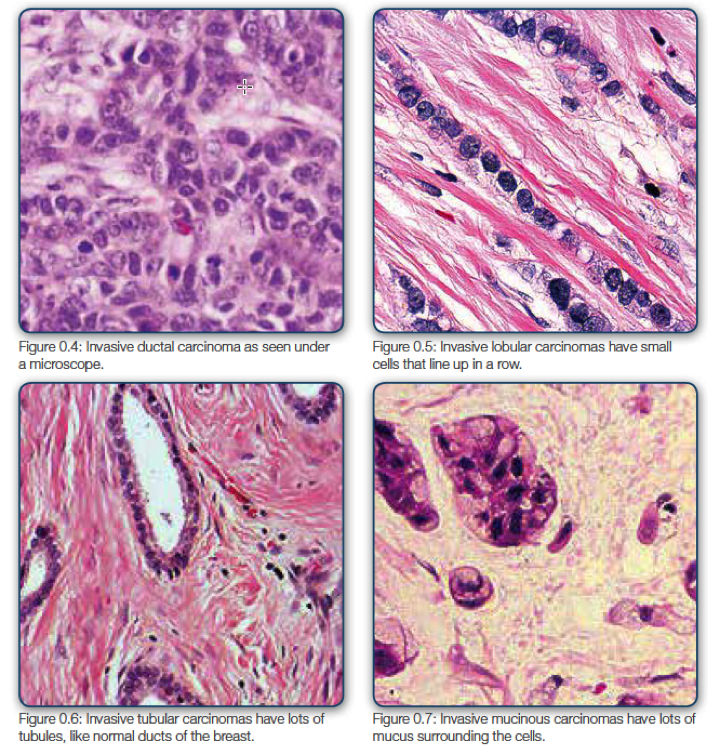
The pathologist will call the invasive carcinomas by different names depending on the pattern of the invasion. The most common type of cancer is an invasive ductal carcinoma (Figure 0.4).
Invasive lobular carcinoma is the second most common type of invasive cancer. It starts off in the lobules, or “leaves,” and has a distinctive pattern (Figure 0.5). Thepathology report may say “single file” because the cells are usually round, uniform in appearance, and lined up as if walking in a line. The unusual thing about lobular cancer is that it does not cause any reaction in the normal tissue. Ductal carcinoma, for example, can cause scarring, which in turn can cause drawing in of the nipple or dimpling of the skin. Lobular carcinomas, on the other hand, are what I call “sneaky”carcinomas. They tend to cause less reaction and thus often go undetected for longer. The good news about lobular cancers is that they tend to be hormone positive or, estrogen receptor positive, opening them up to more treatment options. However,lobular cancers are often hard to detect on a mammogram. So, if you are worried atany time about your breast and the mammogram is normal, insist on an ultrasound or biopsy to be sure.
An invasive tubular carcinoma means that it contains a lot of little tubules (little pipes that look like the normal ducts). Tubular carcinomas are generally discovered through breast screening in very early stages and have an exceptionally good prognosis (Figure 0.6). Mucinous carcinomas have a lot of mucus, which floats around theducts and lobules when the pathologist looks at it through the microscope (Figure 0.7).
Medullary carcinoma is also a special type of infiltrating breast cancer that is noted by its well-defined edge between the tumor and the surrounding normal tissue. It also has some other special features, including the large size of the cancer cells and the presence of immune system cells called lymphocytes at the edges of the tumor. The outlook (prognosis) for this kind of breast cancer is generally better than for the more common types of invasive breast cancer.
Later, in Control Point #11, I will explain the difference between stage and grade. Briefly though, to use my garden example, stage is how far along the four garden patches a weed has travelled (from 1 to 4). Grade actually describes the weed itself. A grade 1 tumor is more ordered and less likely to spread. It’s a bit like a broad leaf weed in the garden, with very little seed, and tends never to come back when you pull it out. A grade 3 tumor, on the other hand, divides more quickly and looks less ordered and more haphazard under the microscope. It’s a bit like one of those annoying onion weeds that have a tendency to come back after you remove them.
What is really important is to take control of the situation by understanding key points of your treatment, or what some people call “your journey.” Some decisions and steps need to take place before any surgery (Part 2), and some can only take place after your surgery (Part 3). I’ll discuss them all.
When a pathologist examines the tissue under a microscope, he or she looks for small clusters of tumor cells that appear to “float” in pools of mucin. The tumor may be made up mostly of mucin, or mostly of cancer cells separated by small amounts of mucin. This is the pink material that a pathologist can see under the microscope as in Figure 0.7.
A “pure” mucinous carcinoma means that at least 90% of the cells are mucinous. They are mainly hormone sensitive and HER2 negative. We call these “special tumours” as although they can be larger than normal they tend not to spread and are less sensitive to chemotherapy. Clare’s tumour was about 3cm in size and the sentinel node was clear.
Clare, at another hospital was advised chemotherapy and specifically came to see me for my opinion. I mentioned to her that my normal approach is to advise radiotherapy to the breast and tamoxifen. I was concerned about the impact of chemotherapy not only on her quality of life but also fertility. Her tumour was on the larger side and most oncologists advise chemotherapy for younger women with tumours over say 1-2cm if they have not spread to the adjacent lymph hones. If her cancer had spread to her axilla (armpit) I would have recommended chemotherapy.
Clare then showed me her own research from the NCCN. She totally knew the topic, I suspect more than most doctors.
The National Cancer Control Network (NCCN) gave the following recommendations:
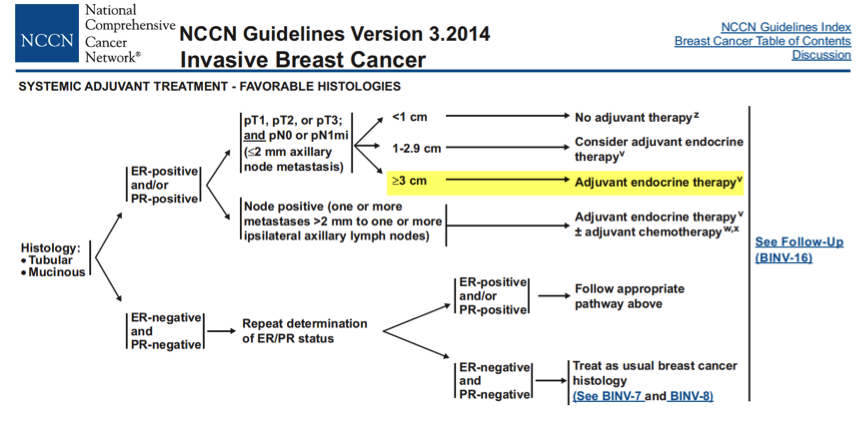
I did mention that chemotherapy could still have a small benefit but at this stage I am leaning towards radiotherapy to the breast and tamoxifen at this stage but for various reasons I sent Clare off for some more tests and also want her case discussed at our MDT team next week.
Breast Cancer: Taking Control is now available at Amazon or at the iTunes store.
John